

The Big Anxiety 2: Breakout My Pelvic Sorcery
In front of me, a red brick wall. Nearer, hovers a large green ball. I hit it. It flies to the wall, knocking out a single brick and bounces back. I hit again. Another brick goes down. But the return is too fast, the ball flies past and I experience a sudden high frequency pulsing in the groin, not exactly painful, but certainly uncomfortable and even moreso each time I miss the ball and the vibrations escalate. I endure for only a few minutes (10 is the maximum), doubling up as what now feels like pain (the ‘cramping’ and ‘hammering’ sensations reported by pelvic pain patients) triggers body memory associated with hernia and prostate operations. The wall and the ball are components of an interactive animation inspired by the Breakout video game. I’m wearing a VR headset and, around my pelvis, a pumped-up inflatable belt holding two nodes to the lower abdomen. I’m spared simulated back pain because, on my visit, the tech is playing up. A blessing.
The work is Eugenie Lee’s Breakout My Pelvic Sorcery, part of The Big Anxiety’s The Empathy Clinic at UNSW Galleries. It’s an artistic creation rooted in solid multidisciplinary science exploring the experience, understanding and communication of chronic pain. Lee’s earlier works focused on externalising and objectifying it, crafting material metaphors with which to manage her own suffering. Now she offers others the opportunity to experience simulacra of chronic pain. At the first Big Anxiety in 2017, I experienced Lee’s Seeing is believing, a VR work conducted within in a padded anechoic chamber. I found myself suspended in a red void with an intensifying, grating soundscape, a barbed wire coil slowly descending around me and finally a large nail passing through the palm of my hand (wired for low-key vibration and heat). A subsequent conversation with the artist, as part of the work, involved putting the unnerving experience into words. The new work has none of the Gothic horror aesthetic of its predecessor, instead the participant is active, attempting to physically and mentally function in a simple physical-virtual game scenario while suffering ongoing and escalating bodily discomfort.
Breakout… is designed to help doctors, nurses and other health and related professionals to understand the nature and impacts of chronic pain: it’s an empathy training machine addressing the suffering regularly experienced by 20% of Australian women and possibly 8% of men. Lee’s collaborators are multidisciplinary, addressing the whole person: Dr Susan Evans (physician, pelvic pain specialist), Emeritus Professor Roland Sussex (linguist, University of Queensland), Dr Claire Ashton-James (social psychologist, empathy expert, University of Sydney), Peter de Jersey (mechatronic engineer), Warren Armstrong (VR media artist) and Big Anxiety producer Bec Dean. Lee has been aided by data from a scientific survey by Sussex, Evans and Ellie Schofield titled The Language of Pelvic Pain, produced by the Pelvic Pain Foundation of Australia.
Empathy: art & transfer of learning
We humans are innately empathetic—without fundamental mutualism, for example, our species would have been short-lived—but for the most part within highly determined cultural boundaries. It is often assumed that education and art in particular loosen those limits by nurturing understanding of others’ emotions and cultures. In recent years, there’s been a preoccupation with the virtues of storytelling, backed by data and theorising of various kinds, but short on an understanding of the transfer of learning required to convert empathy into application, let alone any acknowledgment of the devious narratives inflicted on us every day. The arts can arouse our sympathies, but to what extent? Nigerian-American novelist and essayist Teju Cole, while applauding the risks taken by many of his writer peers, believes only that “literature can save a life. Just one life at a time.” He writes, “After observing the foreign policies of the so-called developed countries, I cannot trust any complacent claims about the power of literature to inspire empathy. Sometimes, even, it seems that the more libraries we have over here, the more likely we are to bomb people over there.”
In her essay “The Banality of Empathy” Zambian writer Namwali Serpell also acknowledges literature’s limits: “Narrative art is indeed an incredible vehicle for virtual experience—we think and feel with characters. It simulates empathy, so we believe it stimulates it.”
Citing Paul Bloom’s complexly argued Against Empathy: The Case for Rational Compassion (Bodley Head, 2016) in which the author argues for cognitive empathy (“understanding what’s happening in other minds and bodies”) over emotional empathy (“trying to feel like or even as someone else”), Serpell writes supportively, “Bloom shows that emotional empathy is often beside the point for moral action. You don’t have to feel the suffocation, the clutch of a throat gasping for air, to save someone [from drowning].” And, as Bloom argues, too much empathy may inhibit a doctor from taking radical action which will induce pain in order to save life.
However, this either-or argument would eliminate Lee’s and a growing number of projects like those encountered in The Empathy Clinic. Surely a synthesis of ‘understanding’ and ‘feeling like’ would be an ideal goal. Pain is intensely private but we constantly share what it is like, comparing another’s with our own experience. The notion that cognitive empathy is somehow free of the traps of emotion seems untenable.
The semantics of pain
One way of coming to understand others’ pain is through attentive listening to the vocabulary and narratives with which sufferers attempt to describe (to themselves, friends, doctors) and take some control of their condition. It’s long been recognised that using metaphor is the commonest means of describing pain (transferring associations from one domain to another). Susan Sontag invaluably challenged the use of metaphor in Illness as Metaphor (1978) for its reduction of the sufferer to Other (clinically and socially objectified in terms of their illness) and the deployment of emotionally negative analogies, especially stigmatising ones to do with cancer. To achieve this, she deployed numerous metaphors herself while, critics argued, denying those in pain the same means of managing it (see Richard Gwyn, Communicating Health and Illness, Sage Publications, 2002, an excellent account of professional medical and patient metaphors and narratives).
For Lee’s Seeing is Believing, psychologist Ronald Melzack’s McGill Pain Questionnaire (1975), which mapped sensory, affective, evaluative and other descriptors used by patients to describe their experience of pain, was a touchstone. However, in Australia Professor Roland Sussex and associates have freshly researched this terrain, surveying over 1000 women about pelvic pain in The Language of Pelvic Pain study, focussing, as Sussex says in a talk, “on the guts of the language itself.” The team discovered, surprisingly, he says, that conjunctive simile usage (eg “a stabbing pain that feels like a hot barb”) was the prevalent means of description.
The researchers also learned that certain sets of similes complemented specific pelvic conditions, be they period, endometrial, ovulation, bladder or vulval pain, the latter, for example, having no “cramping” descriptors common to the other categories, let alone being the most difficult to describe. It was this new study that Lee turned to formulate the kind of discomfort she would induce in her subjects.
The sharability of pain
In her classic work The Body in Pain: The Making and Unmaking of the World (OUP, 1986), Elaine Scarry wrote of the existential “unsharability” of pain and its resistance to language, if not necessarily to art. Pain itself cannot be shared, but the McGill Questionnaire and The Language of Pelvic Pain project point to the capacity of sufferers to use metaphor and simile as a means of sharing expression of their pain and to have their need to be heard acknowledged. It crucially underlines commonalities of experience between sufferers. For health professionals attentive to language this sharing provides indicators of the whereabouts and nature of certain conditions and the qualities of the pain, yielding a rational understanding, Bloom’s ‘cognitive empathy.’ But metaphor is potent; it’s only a short step to the listener drawing on their own experiences of pain to becoming ‘as if’ the sufferer, just as we can have a visceral response to hearing about bodily damage or seeing operation scenes on screen. We can move quickly from understanding to emotional empathy with little or no conscious effort, but to what degree comprehended and how enduring?
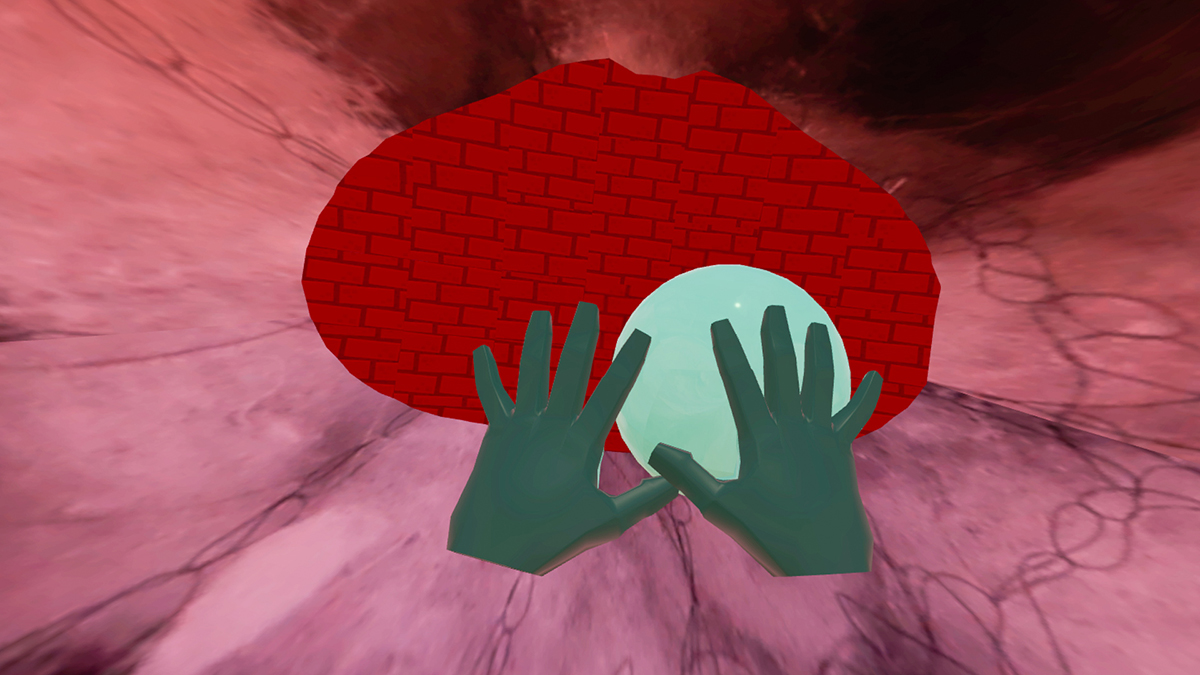
Screenshot of Animation (in development), Breakout My Pelvic Sorcery, Eugenie Lee
Metaphor, magic & science
With her VR translation of sufferers’ metaphors into very convincing simulacra of pain for non-sufferers of pelvic pain, Eugenie Lee synthesises rational understanding and affective experience, most tellingly for me when I attempted to describe what I felt, for a moment completing a loop between myself and those whose suffering prompted the making of Breakout My Pelvic Sorcery. In a video accessible on Lee’s website, gynaecologists testing Breakout My Pelvic Sorcery, speak enthusiastically of the value of the VR’s enabling them to feel something akin to their patients’ suffering.
Like a metaphor, Breakout My Pelvic Sorcery, stands in for and expresses Eugenie Lee’s own experience of pelvic pain as well as for the women who contributed their own metaphors to The Language of Pelvic Language project. Lee’s art is informed and driven by multidisciplinary science. For much of the 20th century, positivist science saw metaphor as being loosely associative, subversive even and having no cognitive value; only literal language would do. The “sorcery” of the work’s title evokes Lee as VR conjurer of ‘pain’ and effector of balm, and a cheeky promulgator of a productive, magical tension between art and science, encouraging a potent dialectic of emotional and cognitive empathies. With further testing and collection of responses from participants, this work-in-progress seems, from my relatively innocent vantage, very promising. As Lee is aware, Breakout My Pelvic Sorcery not will not suit everyone; for some it will seem invasive. But for those happy to brave temporary physical or cultural discomfort it might be a venture into newly found or deeper empathy.
–
The Big Anxiety, first staged in 2017, is a festival that “brings together artists, scientists and communities to question and re-imagine the state of mental health in the 21st century” (website). Artistic and Executive Director Professor Jill Bennett (UNSW), Producer Tanja Farman, Senior Curator Bec Dean.
Breakout My Pelvic Sorcery, artist Eugenie Lee, physician, pelvic pain specialist Dr Susan Evans, linguist Emeritus Professor Roland Sussex, social psychologist, empathy expert Dr Claire Ashton-James, mechatronic engineer Peter de Jersey, VR media artist Warren Armstrong, producer Bec Dean; The Big Anxiety, The Empathy Clinic, UNSW Galleries, Sydney, 23 Sept-9 Nov
Top image credit: Eugenie Lee and Keith Gallasch, Breakout My Pelvic Sorcery, photo © Cynthia Sciberras


